What is Hypophosphatasia?
What is Hypophosphatasia (HPP)?
Hypophosphatasia (HPP) is an ultra-rare, genetic, metabolic, bone and tooth disorder. Although first reported in English medical literature by Dr. Bruce Chown of Manitoba in 1936, HPP was known for many years as Rathbun’s Syndrome, due to it being recognized and named by Dr. J.C. Rathbun of Ontario, in 1948.
Alterations in the TNSALP (tissue nonspecific isoenzyme of alkaline phosphatase) gene lead to low alkaline phosphatase (TNSALP) activity. This form of the enzyme is made in the liver, bone and kidney and is necessary in cell processes for muscle metabolism and to mineralize bones and teeth. This error in metabolism decreases the activity of TNSALP, which results in low levels of tissue and serum TNSALP.
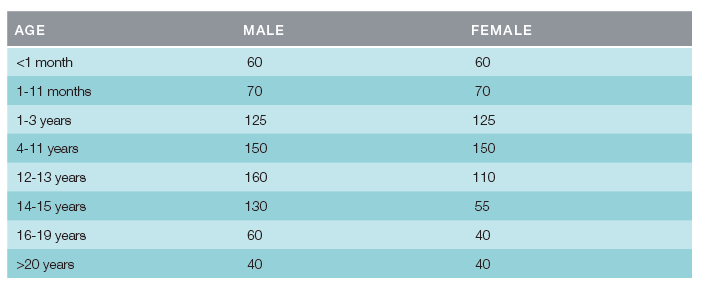
Adapted from: ARUP Laboratories. Alkaline phosphatase isoenzymes, serum or plasma: 0021020. Available at: http://ltd.aruplab.com/tests/pub/0021020
Initial testing includes a serum TNSALP level. If a low TNSALP level is found, together with an elevated plasma pyridoxal 5-phosphate (PLP/vitamin B6) and supporting radiographs, a diagnosis of hypophosphatasia must be considered.
HPP is characterized by a form of rickets (a softening and weakening of the bones), and often a form of osteomalacia (soft bones more likely to bow and fracture than are harder, healthy bones). The defective bone and tooth mineralization can lead to muscle weakness, achy bone pain, fractures, early tooth loss, lack of cementum and cavities due to thin enamel.
This is not the same as osteoporosis, another bone disorder that also can lead to bone fractures. This osteomalacia is resulting from a defect in the bone-building process, while osteoporosis develops due to a weakening of previously constructed bone.
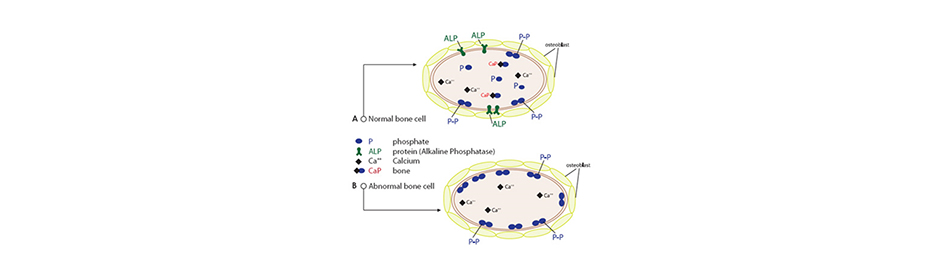
Figure 1 Bone Matrix Normally, bone-forming cells called osteoblasts secrete packets of the enzyme alkaline phosphatase. These packets release phosphate groups from the surface of cells, which then combine with calcium and together deposit in the matrix as “bone crystals,” as shown in diagram A.
The most severely affected will fail to form a mineralized skeleton in the womb and are stillborn. Due to the severity of their condition, the life expectancy for those with perinatal HPP is measured only in days or weeks.
Incidence has been estimated at 1 case per 100,000 live births. Clinical presentation varies widely, from death in the womb to cases in which pathologic fractures first present in adulthood. Incidence of the severe form is believed to be approximately 1 case per 100,000 live births. In some populations, such as Canadian Mennonites, the frequency is as high as 1 case per 2500 newborns.